

Background: The persistence of measurable residual disease (MRD) has been shown to correlate with higher rates of relapse and worse survival in several leukemias. Individual studies have similarly suggested that the detection of MRD is associated with inferior outcomes in patients with acute myeloid leukemia (AML) undergoing frontline therapy; however, the optimal use of MRD information to risk stratify patients and inform clinical decision-making has been limited in part by the heterogeneity of these reports. To better understand the relationship between MRD and clinical outcomes in AML, we performed a literature-based meta-analysis of published AML studies reporting the association of MRD with survival outcomes.
Methods: We conducted independent searches of PubMed, MEDLINE, and Embase for papers published between January 1, 2000 and October 1, 2018 that included the keywords "AML," "acute myeloid leukemia," or "acute myelogenous leukemia," in combination with the keywords "MRD," "minimal residual disease," or "measurable residual disease." Reviews, non-English articles, and studies only reporting outcomes after hematopoietic stem cell transplantation or those with insufficient description of MRD information were excluded. Study sample size, patient age, median follow-up time, MRD detection method, MRD assessment time point(s), AML subtype, specimen source, and survival outcomes were extracted. Meta-analyses of survival probabilities and hazard ratios (HRs) were performed separately for disease-free survival (DFS) and overall survival (OS) using Bayesian hierarchical modeling.
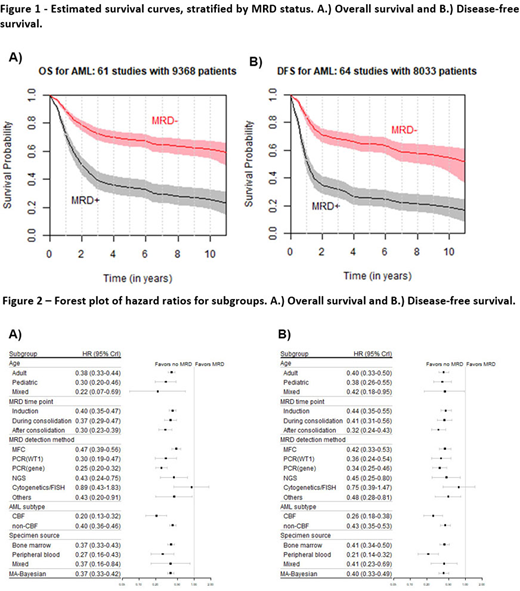
Results: Eighty-one publications reporting on 11,151 patients were included in the meta-analysis (17 studies for OS, 20 studies for DFS, and 44 for both). Both OS and DFS were better for those who achieved MRD negativity (Figure 1). At 5 years, the estimated OS was 68% (95% Bayesian credible interval [CrI], 63%-73%) for the MRD negative group versus 34% (95% CrI, 28%-40%) for the MRD positive group. Similarly, the estimated DFS at 5 years for the MRD negative and MRD positive groups were 64% (95% CrI, 59%-70%) and 25% (95% CrI, 20%-32%), respectively. The relative benefit of achieving MRD negativity was comparable for both OS and DFS (average HR, 0.36; 95% CrI, 0.33-0.39 for OS; average HR, 0.37; 95% CrI, 0.34-0.40 for DFS).
Achievement of MRD negativity was associated with superior DFS and OS irrespective of age group (adult or pediatric), MRD assessment time point (induction, during consolidation or after consolidation), AML subgroup (core-binding factor [CBF] or non-CBF), or specimen source (bone marrow or peripheral blood) (Figure 2). While most of the MRD detection methods were able to identify a difference in DFS and OS between groups with MRD negativity versus MRD positivity, the MRD effect using cytogenetics/FISH was not significant (average HR, 0.77; 95% CrI, 0.39-1.56 for OS and average HR, 0.65; 95% CrI, 0.34-1.23 for DFS), possibly due to only 2 studies being included in this subgroup analysis.
The effect of MRD on survival was more profound in studies reporting outcomes of CBF AML compared to non-CBF AML, with a posterior probability of 0.999 for OS and 0.997 for DFS. Interestingly, across AML subtypes, peripheral blood assessment of MRD better distinguished MRD-positive and MRD-negative groups as compared to bone marrow assessment of MRD, with a posterior probability of 0.918 for OS and 0.999 for DFS.
Multivariate analysis was performed to control for possible confounding factors that might influence the subgroup analyses. Overall, multivariate results were consistent with the univariate results. All subgroups showed DFS and OS benefit to achievement of MRD negativity, with the exception of MRD detection by cytogenetics/FISH.
Conclusions: In this large-cohort meta-analysis, achievement of MRD negativity was strongly associated with superior DFS and OS in patients with AML, an association that was observed across ages, disease subtypes, time of assessment, specimen source, and most MRD detection methods. Given the robustness of the association of MRD with long-term outcomes across studies, MRD status may serve as a valuable clinical endpoint that may allow for accelerated evaluation of novel therapies in AML.
Short:Astellas: Research Funding; Takeda Oncology: Consultancy, Honoraria, Research Funding; AstraZeneca: Consultancy; Amgen: Honoraria. Berry:Berry Consultants LLC.: Other: Co-owner. Walter:StemLine: Research Funding; Selvita: Research Funding; Seattle Genetics: Research Funding; Race Oncology: Consultancy; BioLineRx: Consultancy, Research Funding; Astellas: Consultancy; Arog: Research Funding; Argenx: Consultancy; Aptevo: Consultancy, Research Funding; Amphivena: Current equity holder in publicly-traded company; Amgen: Consultancy, Research Funding; Agios: Consultancy, Research Funding; Jazz: Consultancy, Research Funding; ImmunoGen: Research Funding; Genentech: Consultancy; Daiichi: Consultancy; Celgene: Consultancy, Research Funding; Boston Biomedical: Consultancy; BiVictriX: Consultancy; Pfizer: Consultancy, Research Funding; New Link Genetics: Consultancy; Macrogenics: Research Funding; Kite: Consultancy. Kantarjian:Immunogen: Research Funding; Daiichi-Sankyo: Honoraria, Research Funding; BioAscend: Honoraria; Delta Fly: Honoraria; Abbvie: Honoraria, Research Funding; Ascentage: Research Funding; Novartis: Honoraria, Research Funding; Pfizer: Honoraria, Research Funding; Amgen: Honoraria, Research Funding; Janssen: Honoraria; Oxford Biomedical: Honoraria; Adaptive biotechnologies: Honoraria; Actinium: Honoraria, Membership on an entity's Board of Directors or advisory committees; Sanofi: Research Funding; Aptitute Health: Honoraria; BMS: Research Funding; Jazz: Research Funding. Ravandi:Orsenix: Consultancy, Honoraria, Research Funding; BMS: Consultancy, Honoraria, Research Funding; Macrogenics: Research Funding; Jazz Pharmaceuticals: Consultancy, Honoraria, Research Funding; Amgen: Consultancy, Honoraria, Research Funding; Celgene: Consultancy, Honoraria; Abbvie: Consultancy, Honoraria, Research Funding; Xencor: Consultancy, Honoraria, Research Funding; AstraZeneca: Consultancy, Honoraria; Astellas: Consultancy, Honoraria, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal